Mechanism
VT mechanism falls along a spectrum that maps directly onto patient substrate.
Scar-mediated reentry (ischemic and non-ischemic cardiomyopathy)
- Surviving myocyte bundles within infarct scar form channels of slow conduction
- A wavefront enters the channel, exits the scar border, and reenters — producing stable monomorphic VT
- Most common substrate in clinical practice
- Multiple morphologies common — each reflects a different exit site or channel
Idiopathic VT (structurally normal heart)
- RVOT/LVOT VT: triggered activity from cAMP-mediated delayed afterdepolarizations
- Fascicular VT: reentry involving the left posterior fascicle, verapamil-sensitive
- LBBB inferior axis morphology suggests RVOT; RBBB superior axis suggests fascicular
- Benign prognosis but symptomatic; highly responsive to ablation
Polymorphic VT and torsades
- Long QT: pause-dependent torsades from early afterdepolarizations
- Brugada: phase 2 reentry from transmural repolarization gradient
- Catecholaminergic polymorphic VT (CPVT): RyR2 dysfunction, exercise-triggered
- Ischemic polymorphic VT: acute MI substrate, rarely sustained
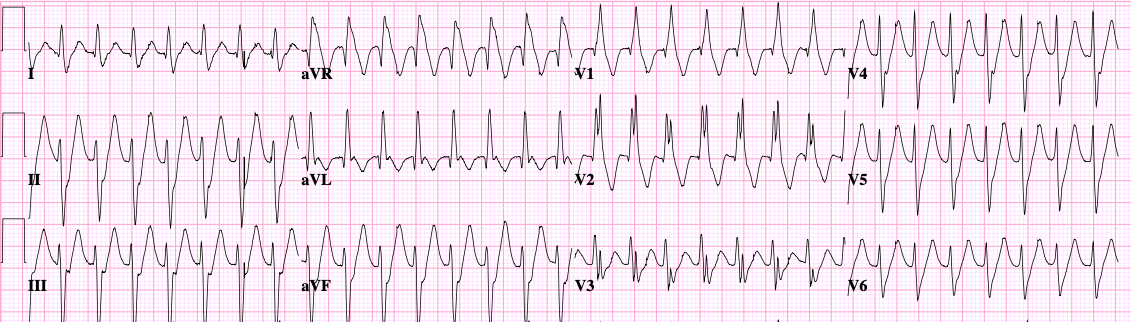
ECG features
When the QRS is wide, default to VT and let the data argue you out of it.
- AV dissociation is the single most specific finding — if you see it, you’re done
- Capture and fusion beats are diagnostic but rare in fast VT
- Concordance (all precordial leads positive or all negative) strongly favors VT
- Brugada algorithm: stepwise approach focusing on RS morphology and intervals
- History trumps ECG: prior MI, EF <35%, or known cardiomyopathy makes VT overwhelmingly likely
Work-up
- 12-lead ECG in tachycardia and sinus rhythm — compare morphologies for scar location
- TTE for EF, wall motion, and structural disease
- Cardiac MRI to characterize scar burden and pattern (subendocardial vs midwall vs epicardial)
- Coronary evaluation — ischemia is a common reversible trigger
- Genetic testing for suspected inherited channelopathies and cardiomyopathies
- EP study for risk stratification in selected patients and as a prelude to ablation
Treatment overview
- Acute management:
- Unstable: synchronized cardioversion
- Stable monomorphic VT: amiodarone, procainamide, or cardioversion
- Polymorphic with QT prolongation: magnesium, overdrive pacing, withdraw offending drugs
- Polymorphic with normal QT: treat ischemia, consider beta-blockers
- Reversible cause search: ischemia, electrolytes (K, Mg), QT-prolonging drugs, decompensated HF
- ICD: secondary prevention after sustained VT/VF in structural heart disease; primary prevention by EF and substrate criteria
- Antiarrhythmics: amiodarone, sotalol, mexiletine — adjuncts to reduce shocks, not curative
- Catheter ablation: increasingly first-line for recurrent monomorphic VT; reduces ICD shocks and improves quality of life
- Stereotactic body radiotherapy is an emerging option for refractory VT
What we do in clinic
- Every VT patient gets a substrate work-up: ECG comparison, echo, often MRI
- We’re aggressive about ischemic evaluation in patients with risk factors — revascularization sometimes meaningfully reduces VT burden
- For ICD recipients with recurrent shocks, we move toward ablation early. Repeated shocks are traumatic and predict worse outcomes; intervention should not wait for a full antiarrhythmic trial.
- Idiopathic VT from RVOT or LVOT is a satisfying diagnosis — ablation is highly successful and patients often come off all medications
- We counsel that scar-mediated VT ablation reduces but rarely eliminates the substrate; an ICD remains important and recurrence is realistic