Mechanism
A macro-reentrant circuit travels around the tricuspid annulus with the cavotricuspid isthmus (CTI) — the strip of tissue between the IVC and the TV annulus — serving as the zone of slow conduction that lets the wavefront re-enter.
- Counterclockwise (~90%): wavefront travels down the lateral RA wall, through the CTI, up the septum, across the roof. Produces negative sawtooth in inferior leads.
- Clockwise (~10%): opposite direction through the same circuit. Inferior leads turn positive.
- The crista terminalis acts as the lateral barrier; the eustachian ridge and TV annulus complete the boundaries.
This is anatomic reentry — fixed obstacles, predictable circuit, ablatable at the bottleneck.
ECG features
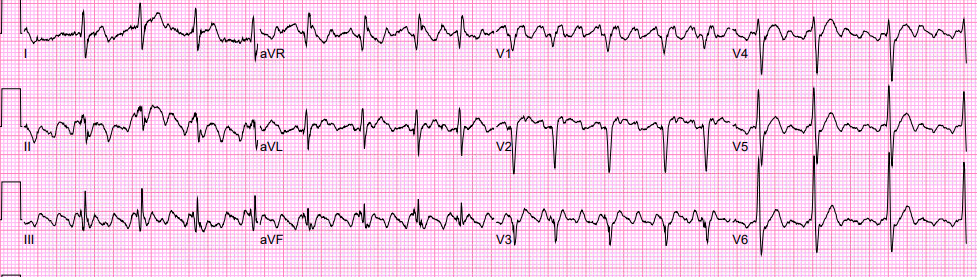
The sawtooth pattern is the headline.
- Inferior leads (II, III, aVF): negative flutter waves with no isoelectric baseline. The continuous undulation distinguishes flutter from AT.
- V1: small positive flutter wave; transitions to negative by V6.
- Atrial rate: 250–350 bpm. Slower on class I or III antiarrhythmics — can drop to 200, raising risk of 1:1 conduction.
- Ventricular rate: 150 bpm in 2:1 conduction is so common that any regular narrow-complex SVT at exactly 150 should prompt a hunt for hidden flutter waves. Carotid massage or adenosine to slow AV conduction reveals them.
Watch for antiarrhythmic-induced 1:1 conduction — a patient started on flecainide or propafenone for AF can develop slow flutter that conducts 1:1, presenting as a wide-complex tachycardia (rate-related aberrancy) at 200+ bpm. Always pair IC drugs with an AV nodal blocker.
Lab setup
Standard catheter configuration for a flutter case:
- Decapolar in the coronary sinus: defines septal activation, provides reference for entrainment.
- Duodecapolar (HALO) around the tricuspid annulus: documents the activation sequence — counterclockwise shows distal to proximal, clockwise the reverse.
- Ablation catheter: irrigated tip, 8 mm tip is an older alternative but irrigated is standard.
- Right ventricular catheter: usually not needed for pure CTI flutter unless concomitant VT or AVN testing planned.
3D mapping (CARTO or EnSite) is helpful for confirming the circuit and documenting block but not mandatory — many operators do CTI flutter with fluoro and the HALO alone.
Ablation
- Target: a continuous lesion from the TV annulus to the IVC across the CTI.
- Approach: pull the catheter back along the isthmus, applying RF in overlapping lesions. Irrigation flow ~17 mL/min, power 30–40 W, contact force 10–20 g.
- Length: roughly 2–3 cm depending on isthmus length, which varies considerably. Pouches and ridges add difficulty.
Endpoints
- Bidirectional block across the CTI — the only acceptable endpoint
- Pace from low lateral RA (just lateral to ablation line) and from CS os; the activation should travel around the line, not across it
- Measure conduction time before and after — significant prolongation supports block
- Differential pacing techniques confirm complete vs incomplete block
- Persistent gap → return to ablation; missed gaps are the #1 cause of recurrence
Practical notes
- Most cases under 90 minutes; many under 60.
- Anticoagulation: bridge with heparin during ablation if not already on DOAC. TEE if in flutter >48 h without therapeutic anticoagulation for the preceding 3 weeks.
- Post-ablation: continue anticoagulation for at least 4 weeks; longer per CHA2DS2-VASc and AF risk.
- Document and counsel about AF — many flutter patients have or will develop AF. Don’t oversell the ablation as definitive for atrial arrhythmia in general.