Mechanism
An accessory pathway (AP) is a strand of myocardium bridging the AV groove that escaped resorption during embryologic development. It conducts independently of the AV node, with its own refractoriness and conduction velocity.
- Manifest AP: conducts antegrade, producing pre-excitation (delta wave) at rest.
- Concealed AP: only conducts retrograde — invisible at rest but available for AVRT.
- Bystander AP: present but not part of the tachycardia circuit (e.g. AVNRT in a WPW patient).
Tachycardia mechanisms
- Orthodromic AVRT (~90%): antegrade down the AV node, retrograde up the AP. Narrow QRS unless aberrancy.
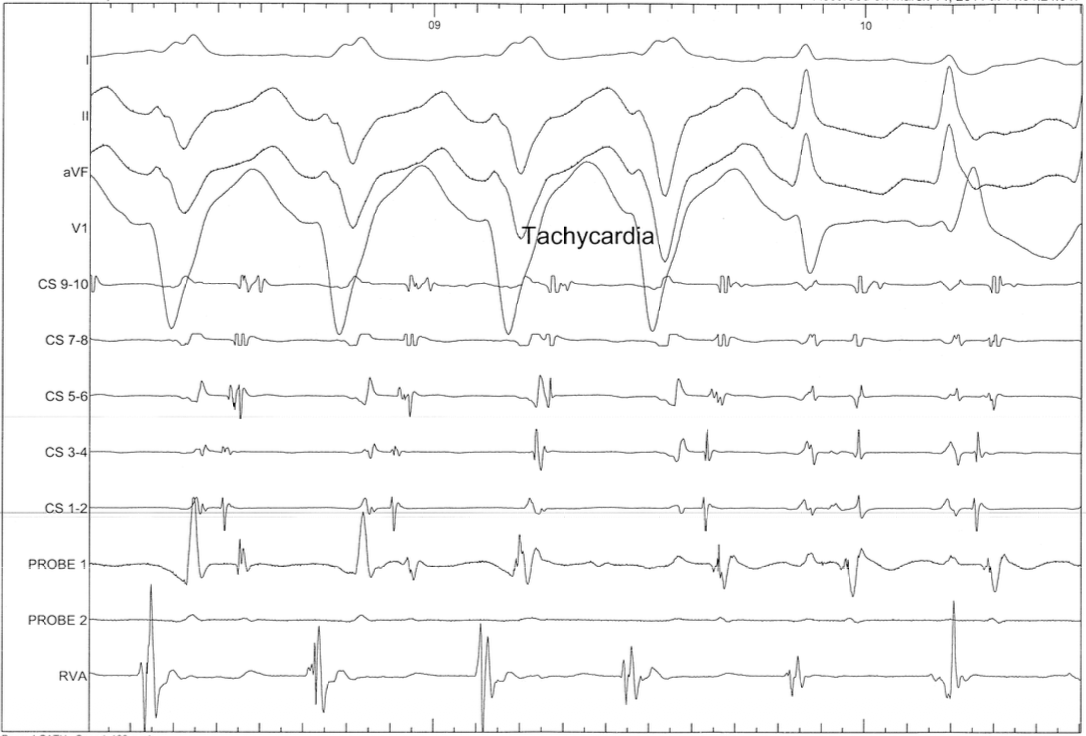
- Antidromic AVRT (~5%): antegrade down the AP, retrograde up the AV node (or another AP). Wide QRS, maximal pre-excitation.
- Pre-excited AF: not reentry — AF conducted to the ventricle through the AP. Look for irregularity and QRS morphology change beat to beat.
ECG features
WPW resting pattern
- PR < 120 ms (short because AP bypasses AV nodal delay)
- Delta wave: slurred upstroke at the start of QRS
- QRS width > 110 ms from the fusion of AP and AV node activation
- Secondary repolarization changes — discordant T waves that can mimic ischemia
Localization
Algorithms like Arruda use delta polarity in specific leads to predict AP location.
- Negative delta in II, III, aVF → posteroseptal or posterior
- Negative delta in I, aVL → left lateral
- Positive delta V1 → left-sided pathway
- Negative or isoelectric delta V1, positive in inferior → right-sided
- Transition zone in precordials also informative
Get a clean 12-lead in sinus with maximum pre-excitation (low-dose adenosine or pacing from the high RA) before mapping.
Risk stratification of WPW
Most pre-excitation is benign, but a minority of patients have rapid AP conduction that allows pre-excited AF to degenerate into VF. Sudden death risk is ~1 in 1000 patient-years overall, higher in symptomatic patients.
- Non-invasive markers of low risk: intermittent pre-excitation, loss of delta with exercise, loss with procainamide challenge
- EP study indications: symptomatic patients, competitive athletes, high-risk occupations, any history of AF or syncope
- Invasive risk markers:
- Shortest pre-excited RR in induced AF (SPERRI) — <250 ms concerning, <220 ms high risk
- AP effective refractory period <250 ms
- Multiple pathways
- Inducible AVRT
Asymptomatic WPW in adults is increasingly being studied invasively because the risk markers are not reliably predicted from the surface ECG alone.
EP study and ablation
- Mapping: earliest ventricular activation in tachycardia or during atrial pacing for antegrade APs; earliest atrial activation during ventricular pacing or orthodromic AVRT for retrograde mapping.
- Left-sided pathways: transseptal or retrograde aortic. Map along the mitral annulus.
- Right-sided pathways: femoral venous access, map the tricuspid annulus. Right free wall is harder — annulus is mobile and contact is unstable.
- Posteroseptal: check the CS for a CS diverticulum, which harbors epicardial pathways requiring ablation inside the venous structure.
- Para-Hisian pathways: cryo preferred for reversibility.
Endpoints
- Loss of pre-excitation with confirmation of decrement and VA block at the AV node
- Non-inducibility of AVRT on isoproterenol with and without atropine
- AP ERP > 250 ms if not eliminated (rare scenario, usually we ablate)
Practical notes
- Wide-complex tachycardia in a young patient with no structural disease — think antidromic AVRT or pre-excited AF before VT.
- Acute pre-excited AF: procainamide or ibutilide, avoid adenosine, verapamil, diltiazem, digoxin, beta-blockers. Cardiovert early.
- Document the resting pre-excitation pattern in the chart before ablation — post-ablation ECG should look normal.