Mechanism
AVNRT lives in the AV junction, not the AV node itself in any clean anatomic sense. Two regions with different conduction properties form the substrate.
- Slow pathway: posterior input near the CS os, short refractory period, slow conduction. Travels along the tricuspid annulus.
- Fast pathway: anterior/superior input near the apex of Koch’s triangle, fast conduction, long refractory period.
- A PAC blocks in the fast pathway (still refractory), conducts antegrade down the slow pathway, and by the time it reaches the lower common pathway the fast pathway has recovered — retrograde conduction up the fast pathway completes the loop. The classic “PR jump” on initiation is the giveaway.
Typical vs atypical
- Typical (slow-fast): antegrade slow, retrograde fast. Short RP. Retrograde P buried in or just after the QRS.
- Atypical (fast-slow): antegrade fast, retrograde slow. Long RP, mimics AT. Deeply negative inferior Ps.
- Slow-slow: rare variant using two slow inputs. Intermediate RP.
ECG features
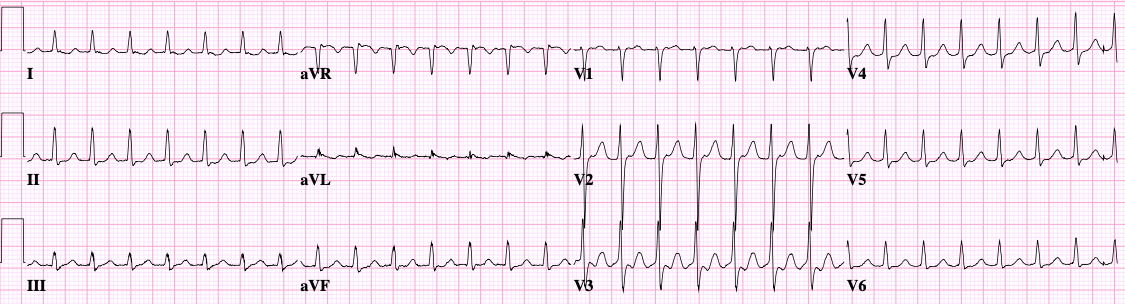
Lead V1 and the inferior leads do most of the diagnostic work.
- Pseudo-r’ in V1 — a terminal positive deflection in QRS that wasn’t there in sinus rhythm.
- Pseudo-S in II/III/aVF — a notch on the downslope of the QRS, the same retrograde P viewed from below.
- Compare to a baseline sinus ECG whenever possible; the “pseudo” findings are only visible by comparison.
- RP < 70 ms strongly favors AVNRT over AVRT.
- Onset captured on monitor: a sudden long PR followed by tachycardia is the slow pathway jump.
Maneuvers and adenosine
- Vagal maneuvers (Valsalva, modified Valsalva with leg lift, carotid sinus massage) terminate ~25–50%.
- Adenosine 6 mg IV push followed by saline flush, escalate to 12 mg. Termination is diagnostic and therapeutic.
- Watch the monitor during adenosine: termination on a P wave (block in slow pathway) is classic for AVNRT. Termination on a QRS without a following P also fits.
- If tachycardia persists despite AV block — think AT or flutter.
EP study findings
- Dual AV nodal physiology: AH jump of ≥50 ms with a 10 ms decrement of A1A2.
- Echo beats during programmed stimulation.
- Earliest atrial activation during tachycardia at the His or just posterior to it (typical), or at the CS os (atypical).
- VA interval ≤70 ms on His electrogram in typical.
- Para-Hisian pacing distinguishes from septal AP — nodal pattern in AVNRT.
- Entrainment from RV: V-A-V response (rules out AT), corrected post-pacing interval and SA-VA interval support AVNRT over AVRT.
Ablation
- Target: slow pathway, anterior approach into Koch’s triangle. Map between the CS os and the tricuspid annulus along the septal TV.
- Anatomic landmarks: CS os posteriorly, His anterosuperiorly, TV annulus laterally. The compact AV node sits at the apex — stay away.
- Energy: RF 30–50 W titrated. Cryoablation in young patients or anatomy close to His for reversibility.
- Endpoints: elimination of slow pathway conduction or a single residual echo beat with no sustained tachycardia on isoproterenol with and without atropine.
- Junctional beats during RF mean you’re on the slow pathway — monitor VA conduction during every junctional. Loss of VA or fast junctional without retrograde P means stop immediately.
Practical lab notes
- Most cases are quick — diagnostic study plus ablation in 60–90 minutes.
- Femoral access only; no transseptal needed.
- Most patients walk out the same day.
- Recurrence is uncommon (<5%) but typically presents within the first 3 months.